7 Crucial Facts About Zombie Cells – Their Role in Aging Diseases
Table of Contents
Zombie cells, scientifically known as senescent cells, represent a fascinating and increasingly critical area of research in the quest to understand and combat aging and its associated diseases. These unique cells are characterized by a permanent halt in cell division, a state they enter typically in response to damage such as DNA breaks, telomere shortening, or oxidative stress. Unlike cells that undergo programmed cell death (apoptosis) and are cleanly cleared from the body, senescent cells persist, remaining metabolically active and refusing to die. This resistance to clearance, coupled with their detrimental secretions, has earned them the evocative moniker “zombie cells” because, much like the undead in popular culture, they refuse to die when they should and actively spread harm to their surroundings.
The accumulation of these zombie cells is now recognized as a fundamental hallmark of biological aging. While in younger individuals, the immune system is highly effective at identifying and eliminating these damaged cells, this efficiency declines with advancing age. As a result, senescent cells begin to accumulate in various tissues and organs throughout the body, setting the stage for a cascade of detrimental effects that contribute significantly to the development and progression of numerous age-related conditions. Understanding the intricate mechanisms by which these cellular entities contribute to disease and exploring strategies to mitigate their impact holds immense promise for promoting healthier aging and extending human healthspan.
Understanding Senescent Cells: The ‘Zombie’ Phenomenon
Cellular senescence is a complex biological process initiated when a cell experiences irreparable damage or excessive stress. Instead of undergoing apoptosis (programmed cell death), which would safely remove the damaged cell, the cell enters a state of stable and irreversible cell cycle arrest. This means the cell stops dividing but continues to live. The concept of cellular senescence was first described in 1961 by Leonard Hayflick and Paul Moorhead, who observed that human fetal fibroblasts had a limited number of replications before entering a non-dividing state, a phenomenon now known as the Hayflick limit.
The triggers for senescence are diverse and include genomic instability, telomere attrition (the shortening of protective caps on chromosomes with each cell division), oncogene activation (genes that can promote cancer), oxidative stress, and mitochondrial dysfunction. Once a cell becomes senescent, it undergoes profound phenotypic and functional changes. Morphologically, senescent cells often become enlarged and flattened. Crucially, their gene expression patterns are significantly altered, leading to the production and secretion of a variety of bioactive molecules that collectively form the senescence-associated secretory phenotype (SASP).
The term “zombie cell” vividly captures the paradoxical nature of senescent cells. They are alive but dysfunctional, resisting the natural process of self-elimination. Instead, they linger, consuming resources, and actively exerting harmful effects on their cellular neighborhood. This accumulation, unchecked by an aging immune system, transforms these formerly protective cells into drivers of chronic inflammation and tissue damage, playing a central role in the decline associated with aging.
The Senescence-Associated Secretory Phenotype (SASP): Fueling Inflammation
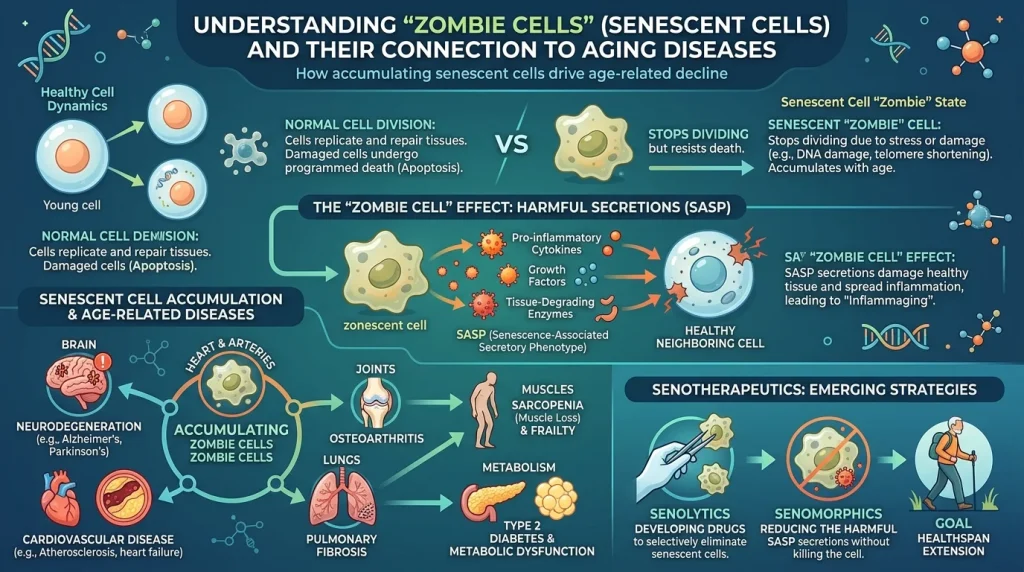
A defining and arguably the most detrimental characteristic of senescent cells is their development of the Senescence-Associated Secretory Phenotype (SASP). The SASP is a complex and heterogeneous collection of molecules that senescent cells continuously release into their surrounding microenvironment. This “toxic cocktail” typically includes pro-inflammatory cytokines (such as IL-6, IL-8, IL-1α, and TNF-α), chemokines (which recruit immune cells), growth factors, and proteases (enzymes that degrade the extracellular matrix). The precise composition of the SASP can vary depending on the cell type, the initiating stimulus for senescence, and the stage of senescence.
The SASP is not merely a passive byproduct of cellular dysfunction; it is an active driver of age-related pathologies. Its primary impact stems from its ability to create a persistent, low-grade inflammatory state, often termed “inflammaging,” which is a hallmark of aging itself. This chronic inflammation damages healthy cells, disrupts tissue homeostasis, and impairs the body’s regenerative capacity.
Specifically, the SASP contributes to harm in several ways:
- Propagation of Senescence: The inflammatory factors released by senescent cells can induce senescence in neighboring healthy cells, a process known as secondary or bystander senescence. This amplifies the impact of a relatively small number of zombie cells, spreading the damage across entire tissue compartments.
- Impaired Stem Cell Function: SASP factors directly disrupt stem cell niches, altering differentiation signals and reducing the proliferative capacity of tissue-resident stem cells. This contributes to the progressive decline in tissue repair and regeneration seen with aging.
- Tissue Degradation and Fibrosis: Proteases secreted as part of the SASP degrade the extracellular matrix, while growth factors can promote fibrosis (scarring), further impairing tissue function.
- Metabolic Dysfunction: SASP factors, such as IL-6, can induce insulin resistance in surrounding tissues, contributing to metabolic dysfunction that worsens with age.
The continuous action of the SASP transforms senescent cells from passive non-dividers into active contributors to systemic inflammation and tissue dysfunction, underscoring their critical role in age-related diseases.
The Dual Nature of Senescence: Protective Roles vs. Detrimental Accumulation
While the narrative surrounding “zombie cells” often emphasizes their harmful aspects, it is crucial to recognize that cellular senescence is not inherently detrimental. In fact, it serves vital protective roles, particularly earlier in life. One of its most significant beneficial functions is as a potent tumor-suppression mechanism. When a cell sustains damage that could potentially lead to uncontrolled proliferation and cancer, senescence acts as an emergency brake, permanently halting its division. This prevents the replication of potentially cancerous cells, thus guarding against tumor formation.
Beyond cancer prevention, senescent cells also play a constructive role in wound healing and tissue repair. During injury, the temporary presence of senescent cells can help limit fibrosis and assist in tissue regeneration by secreting factors that promote repair and attract immune cells to clear debris. This initial beneficial phase is a testament to the complex and context-dependent nature of cellular senescence.
However, the delicate balance shifts with age. In younger individuals, the immune system is highly efficient at detecting and eliminating these transiently senescent cells once their protective job is done. But as the immune system’s surveillance declines with age, senescent cells evade clearance and begin to accumulate in various tissues. It is this chronic accumulation and the sustained release of the SASP that transform their temporary protective role into a persistent, harmful influence.
This dual nature highlights a critical challenge for anti-aging research: developing precision therapies that target only the harmful senescent cell populations without interfering with those that retain beneficial functions. Scientists are increasingly realizing that not all “zombie cells” are bad, and some may actually help keep the body healthy. The goal is to selectively remove the detrimental “rogue” senescent cells without disrupting the body’s natural repair systems or beneficial cellular processes. This nuanced understanding is shaping the next generation of anti-aging interventions.
Zombie Cells and Their Widespread Impact on Age-Related Diseases
The persistent presence and inflammatory secretions of zombie cells are now recognized as a significant contributor to the pathophysiology of a vast array of age-related diseases. Their accumulation acts as a common underlying mechanism, linking cellular aging to systemic health decline.
| Disease Category | Specific Conditions Linked to Zombie Cells | Mechanism of Action by Zombie Cells (SASP) |
|---|---|---|
| Cardiovascular Diseases | Atherosclerosis, heart failure, arterial stiffening, heart attack recovery impairment. | Chronic inflammation, endothelial dysfunction, promotion of plaque instability, increased scar tissue formation in heart muscle. |
| Neurodegenerative Diseases | Alzheimer’s disease, Parkinson’s disease, tauopathies, age-related cognitive decline, neuronal death. | Neuroinflammation, impaired neuronal and glial function (astrocytes, microglia), propagation of tau protein tangles, disruption of neural networks. |
| Metabolic Disorders | Type 2 Diabetes, insulin resistance, obesity, non-alcoholic fatty liver disease (NAFLD) / metabolic dysfunction-associated steatohepatitis (MASH). | Induction of insulin resistance, chronic inflammation in adipose tissue, accumulation of senescent macrophages in the liver, leading to liver scarring and inflammation. |
| Musculoskeletal Conditions | Osteoarthritis, bone degeneration, osteoporosis, muscle weakness, sarcopenia (age-related muscle loss). | Tissue degradation, chronic inflammation in joints, impaired tissue repair, reduced regenerative capacity, affecting bone and muscle integrity. |
| Other Chronic Conditions | Pulmonary fibrosis, chronic kidney disease, tissue fibrosis, impaired wound healing, certain cancers (complex role). | Systemic inflammation, tissue remodeling, disruption of tissue microenvironments, reduced organ function, and in some contexts, promotion of tumor growth. |
In the cardiovascular system, senescent cells contribute to atherosclerosis by promoting inflammation and plaque instability. They also impair heart function after events like heart attacks by increasing inflammation and scar tissue. Research has shown that eliminating zombie cells can improve the reparative properties of human heart cells.
For neurodegenerative diseases, such as Alzheimer’s and Parkinson’s, the accumulation of senescent cells, particularly in specialized brain cells like astrocytes and microglia, leads to chronic neuroinflammation and oxidative stress. This, in turn, impairs neuronal function, causes brain cell loss, and contributes to cognitive decline and memory impairment. Early findings from Mayo Clinic researchers indicated that senescent cells accumulate in certain brain cells prior to cognitive loss, and their removal diminished tau protein aggregation and memory loss in mouse models.
Metabolic disorders are also heavily influenced by zombie cells. They contribute to Type 2 Diabetes and insulin resistance through SASP factors that induce metabolic dysfunction. Recent findings also link senescent macrophages in the liver to metabolic dysfunction-associated steatohepatitis (MASH), a severe form of fatty liver disease, demonstrating that excess cholesterol can push these immune cells into a permanently inflamed state. Clearing these cells in mice was shown to reverse liver damage, even without dietary changes.
Furthermore, senescent cells contribute to musculoskeletal issues like osteoarthritis and osteoporosis by driving inflammation and hindering tissue repair in joints and bones. They also play a role in pulmonary fibrosis, chronic kidney disease, and general age-related decline, including frailty and impaired wound healing. The widespread impact of zombie cells underscores their central role in the overall aging process and the development of multiple chronic diseases.
Targeting Zombie Cells: The Emergence of Senolytics and Senomorphics
Given the profound connection between senescent cells and age-related diseases, scientists are actively developing therapeutic strategies, collectively known as senotherapeutics, to mitigate their harmful effects. These interventions primarily fall into two main categories: senolytics and senomorphics.
Senolytics are a class of drugs specifically designed to selectively induce apoptosis, or programmed cell death, in senescent cells. By eliminating these “zombie cells,” senolytics aim to reduce their burden in tissues and alleviate the detrimental effects of their SASP. This approach directly targets the accumulation problem. Notable senolytic compounds include Dasatinib, a chemotherapy drug, and Quercetin, a plant-derived flavonoid. The combination of Dasatinib and Quercetin has shown promise in preclinical and early clinical studies, effectively clearing senescent cells and improving various age-related conditions in animal models. Other senolytics under investigation include Fisetin and Navitoclax. The goal of senolytics is to prevent, delay, and potentially reverse the signs of aging by enhancing immunity and clearing senescent cells.
In contrast, senomorphics do not kill senescent cells but instead modulate their behavior, specifically by suppressing the harmful components of the SASP. These compounds aim to reduce inflammation, restore tissue homeostasis, and promote tissue regeneration by modifying the environment created by senescent cells. Senomorphics essentially make senescent cells “less harmful” without eliminating them, offering a potentially safer long-term strategy by dampening systemic inflammation. Examples of senomorphic agents include Rapamycin, Resveratrol, Metformin, and Apigenin, which have shown the ability to reduce the harmful effects of the SASP in preclinical studies.
Beyond these two main approaches, researchers are also exploring other strategies. These include combination therapies, which might involve using a senolytic to reduce senescent cell burden and a senomorphic to manage any remaining SASP. Immune-based approaches, such as immunotherapies and senolytic vaccines targeting specific surface antigens on senescent cells, are also gaining attention. Furthermore, lifestyle interventions like regular exercise, a healthy diet, and adequate sleep have been identified as natural modulators that can prevent the accumulation and even promote the clearance of senescent cells, highlighting the importance of holistic health practices in mitigating the impact of these cells.
Advancements and Challenges in Senotherapeutic Clinical Trials
The promising preclinical results of senolytics and senomorphics in animal models, where the removal of senescent cells has led to measurable improvements in tissue function, delayed onset of age-related disorders, and extended healthspan, have spurred a rapid expansion of research into human clinical trials. Over 30 clinical trials are currently completed, underway, or planned, investigating senotherapeutic agents for a variety of conditions ranging from idiopathic pulmonary fibrosis and cardiovascular disease to neurodegenerative disorders like Alzheimer’s and Parkinson’s, metabolic diseases, and musculoskeletal issues like osteoporosis.
Early-phase clinical trials have shown promising initial results regarding the safety and tolerability of certain senolytic compounds in humans. For instance, a Phase I trial investigating the combination of Dasatinib and Quercetin in patients with early-stage Alzheimer’s disease found the treatment to be safe and well-tolerated, and previous research had shown it cleared senescent brain cells in mouse models. These studies are crucial in establishing the foundational safety profile necessary for larger, efficacy-focused trials. Similarly, research is exploring whether senolytic drugs applied topically to the skin could improve overall health by addressing skin senescence, which has been found to influence aging in other parts of the body.
Despite these exciting advancements, several challenges remain in translating senotherapeutic research into widespread clinical practice. One significant hurdle is the heterogeneity of senescent cells. Not all senescent cells are the same; their characteristics, the specific SASP they produce, and their roles can vary greatly depending on the tissue, cell type, and the initial trigger for senescence. This complexity means that a “one-size-fits-all” approach to eliminating senescent cells might not be optimal and could even interfere with the beneficial roles some senescent cells play, such as in wound healing or tumor suppression. Precision anti-aging therapies aim to remove only the harmful “zombie” cells without disrupting the body’s natural repair systems.
Other challenges include reliably identifying senescent cells in vivo, determining optimal treatment windows, understanding the central nervous system penetrance and selectivity of compounds, and evaluating long-term safety considerations, particularly in aged or diseased populations. Researchers are working on developing biomarkers to better track senescent cell burden and therapeutic efficacy. The development of targeted delivery methods and strategies to differentiate between beneficial and harmful senescent cell populations are critical areas of ongoing research. As the scientific community addresses these complexities, the potential for senotherapeutics to revolutionize the treatment of age-related diseases remains a powerful motivation. For more detailed insights into the senescence-associated secretory phenotype, its components, and implications, one can refer to authoritative resources such as Wikipedia’s article on SASP.
Conclusion: Towards a Future of Healthier Aging
The emergence of “zombie cells,” or senescent cells, as a significant driver of aging and age-related diseases marks a paradigm shift in our understanding of longevity and healthspan. These cells, characterized by their permanent cessation of division and the secretion of a harmful inflammatory cocktail known as the Senescence-Associated Secretory Phenotype (SASP), accumulate with age and contribute to a wide spectrum of chronic conditions, from cardiovascular and neurodegenerative diseases to metabolic disorders and musculoskeletal degeneration.
While senescence can play protective roles, particularly in preventing cancer, its chronic presence due to impaired immune clearance in older age becomes a detrimental force. The scientific community’s growing understanding of these cellular mechanisms has paved the way for innovative therapeutic strategies, notably senolytics (drugs that selectively kill senescent cells) and senomorphics (compounds that suppress their harmful secretions).
With numerous clinical trials underway, the potential of senotherapeutics to extend healthy lifespan and prevent or delay multiple age-related diseases simultaneously is a beacon of hope. Although challenges remain, including the need for greater specificity, safety, and a deeper understanding of senescent cell heterogeneity, the ongoing research promises to unlock new avenues for intervention. By targeting these cellular undead, we are moving closer to a future where aging can be a process of healthy longevity, free from the pervasive burden of age-related illnesses. The insights gained from studying zombie cells are not just about adding years to life, but crucially, adding life to years.